Preliminary study of real-time imaging for MR guided intervention and image quality assessment
编号:129
稿件编号:56 访问权限:仅限参会人
更新:2021-11-04 10:05:45 浏览:2281次
张贴报告

摘要
Background: Interventional MRI has significant benefits for image-guided intravascular intervention surgery and related vascular procedures. Compared with X-ray fluoroscopy, MR provides excellent contrast of the vessel wall and surrounding tissue, and have advantages of multi-parameter imaging, no use of contrast agents and no ionizing radiation hazards. In this study, we evaluate the image quality of real-time sequences, fast low angle shot (FLASH) and true fast imaging with steady-state precession (True FISP), for MR compatible guide wire and balloon imaging on a 3.0T MRI scanner.
Methods: All images was performed on Siemens MR guided intervention system, which consists of a 3.0T MR-scanner (Skyra, Siemens, Berlin Germany) and MRI compatible monitor (Fuqing Medical Technology Co., Ltd, Hefei, Anhui, China) . All experiments were conducted using a Peripheral Balloon Catheter (PTA35-6040B, DK MEDTECH, Suzhou, Jiangsu, China) filled with a dilution of 1% of Gadodiamide (for good contrast of balloon, Gadodiamide was injected and only existed in the balloon.) mixed with normal saline (0.8ml) and using magnetic resonance compatible guide wire (diameter=0.035", length=150cm) (EPflex, Dettingen an der Erms, Germany). Guide wire consists of a high-strength para-aramid synthetic fiber core, surrounded by a bending-resistant high performance polymer and a hydrophilic coating, the markers in the guide wire are discretely mosaicked for navigation. All experiments were simulated in a 3D printed aorta phantom printed by 3D printer (SPS250j, Shanxi Hengtong Intelligent Machine Co., Ltd.). The aorta phantom was printed using CTA data from a normal adult and made of transparent resin. The interventional procedure was guided and recorded by FLASH and True FISP. The parameters of the real-time imaging sequence were: (1)FLASH, TR/TE =6.8/2.65ms, FA=12º, FOV=360×147×10mm, Slice thickness=10mm, Phase partial Fourier=6/8, bandwidth=230Hz/Px, temporal resolution=2f/s, (2)True FISP, TR/TE =321.35/1.88ms, FA=49º FOV=360×144×10mm, Slice thickness=10mm, bandwidth=1116Hz/Px, temporal resolution=2f/s.
The real-time image were evaluated objectively and subjectively. For objective scoring, the image signal-to-noise ratio (SNR), contrast noise ratio (CNR), geometric distortion and image uniformity obtained by the two sequences were measured. The signal intensity and noise at different positions of the image were measured and their average value was taken to calculate the SNR. The SNR is calculated by:
SNR=Signalnormal saline/SDnoise. The CNR between gadolinium-filled balloon and normal saline in the phantom was measured. The CNR is calculated by: CNR=|Signalballoon-Signalnormal saline|/SDnoise. Regarding image uniformity, most areas of multiple images were measured, and the average value of their uniformity was calculated. The image uniformity is calculated by: U={1-(Signalmax-Signalmin/Signalmax+Signalmin)}*100%. In terms of geometric distortion, measure the actual length of the gadolinium balloon and its length in the image, and then calculate the geometric distortion. The geometric distortion is calculated by: GD=|Lengthimage-Lengthactual|/Lengthimage*100%.
Subjective scoring of two sequences, Likert scoring method was applied to assess the image sharpness, image distortion and artifacts of all sequences. The images were scored by two experienced radiologists with more than six-year practice. The evaluation criteria were as follows: 1 points = poor image sharpness with serious distortion or artifacts, 2 points = medium image sharpness with medium distortion or artifact, 3 points = good image sharpness with slight distortion or artifacts, 4 points = excellent image sharpness with no distortion or artifacts. Independent sample T-test was used to analyze the scores of subjective evaluation.
Results: Both sequences temporal resolution was 2 frames/s and spatial resolution was 1.1×1.1×10mm. For objective assessment, the two sequences (FLASH vs True FISP) did show significant difference in SNR (102±16 vs 618±137, p<0.05) and CNR (73.5±18 vs 162.2±46,p<0.05). Image uniformity (80%±6% vs 74%±4%, p=0.133) and geometric distortion (2%±1%, 2%±1%) did not show significant difference. Subjective scoring showed that two radiologists reached agreement on the score after discussion, the subjective scores of the two groups of images did show significant difference, and the FLASH score is slightly higher than the True FISP score (FALSH=3.7±0.5, True FISP=3.1±0.9, P=0.03).
Conclusions: Both sequences have sufficient signal-to-noise ratio, contrast to noise ratio, image uniformity and the degree of geometric distortion is also within the acceptable range. The FLASH sequence has sufficient signal-to-noise ratio, and has sufficient guiding ability in the actual application process, the MR-compatible guide wire has moderate size of the marker artifact, and the balloon imaging effect is excellent. The True FISP sequence has higher signal-to-noise ratio and contrast-to-noise ratio, but the markers of the MR-compatible guide wire are marked with excessive artifacts, which affects the visualization of balloon and the vessel wall. The result of subjective evaluation shows that the FLASH sequence has a higher score than the True FISP sequence. Finally, the study shows that FLASH sequence has better guiding ability and effect compared with True FISP.
Fig.1
a-c: image of FLASH, a: guide wire, b: guide wire + balloon with Gd, c: balloon with Gd.
d-f: image of True FISP, d: guide wire, e: guide wire + balloon with Gd, f: balloon with Gd.
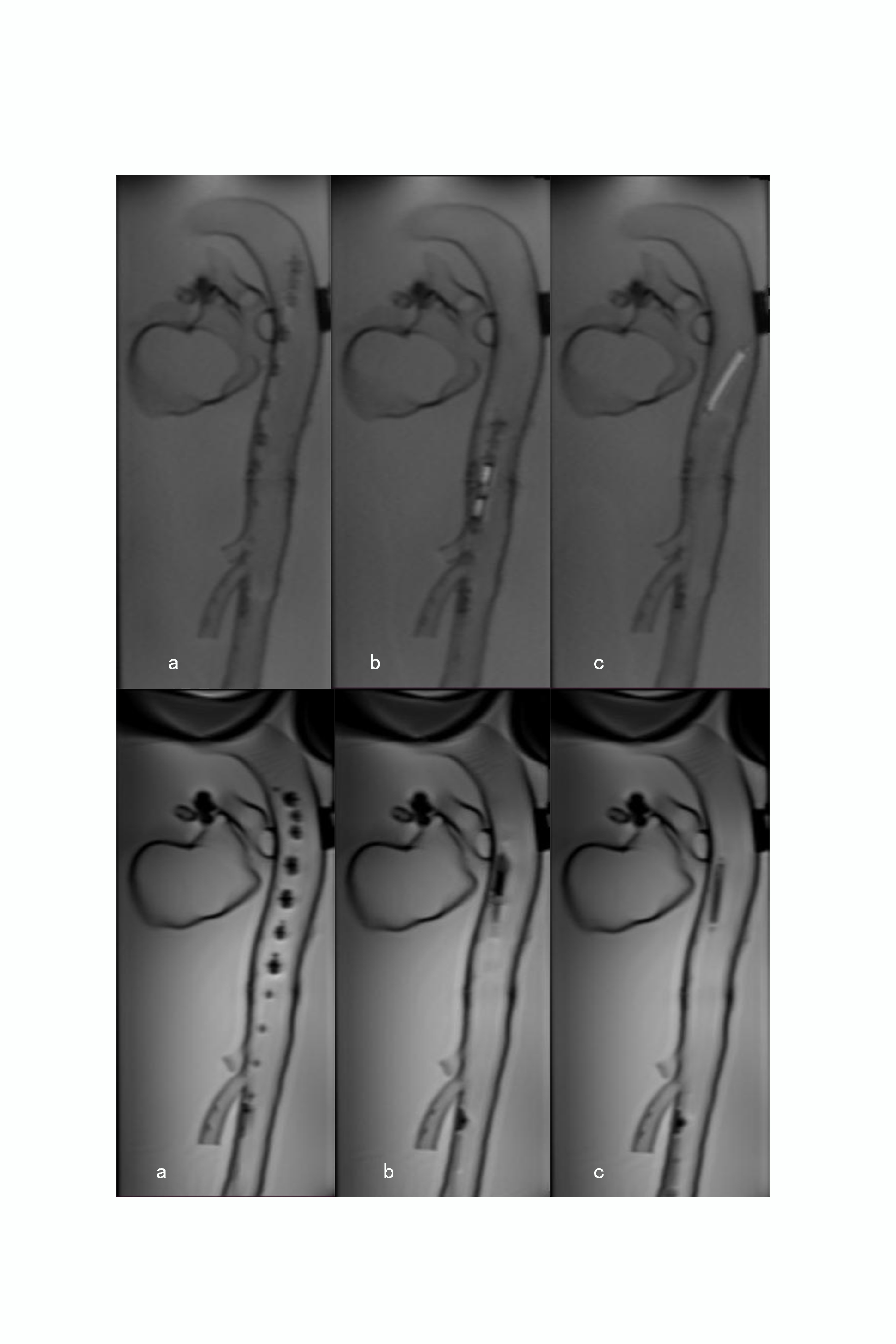
Fig.2
A: aorta phantom, B: balloon, C: MR compatible guide wire.

Methods: All images was performed on Siemens MR guided intervention system, which consists of a 3.0T MR-scanner (Skyra, Siemens, Berlin Germany) and MRI compatible monitor (Fuqing Medical Technology Co., Ltd, Hefei, Anhui, China) . All experiments were conducted using a Peripheral Balloon Catheter (PTA35-6040B, DK MEDTECH, Suzhou, Jiangsu, China) filled with a dilution of 1% of Gadodiamide (for good contrast of balloon, Gadodiamide was injected and only existed in the balloon.) mixed with normal saline (0.8ml) and using magnetic resonance compatible guide wire (diameter=0.035", length=150cm) (EPflex, Dettingen an der Erms, Germany). Guide wire consists of a high-strength para-aramid synthetic fiber core, surrounded by a bending-resistant high performance polymer and a hydrophilic coating, the markers in the guide wire are discretely mosaicked for navigation. All experiments were simulated in a 3D printed aorta phantom printed by 3D printer (SPS250j, Shanxi Hengtong Intelligent Machine Co., Ltd.). The aorta phantom was printed using CTA data from a normal adult and made of transparent resin. The interventional procedure was guided and recorded by FLASH and True FISP. The parameters of the real-time imaging sequence were: (1)FLASH, TR/TE =6.8/2.65ms, FA=12º, FOV=360×147×10mm, Slice thickness=10mm, Phase partial Fourier=6/8, bandwidth=230Hz/Px, temporal resolution=2f/s, (2)True FISP, TR/TE =321.35/1.88ms, FA=49º FOV=360×144×10mm, Slice thickness=10mm, bandwidth=1116Hz/Px, temporal resolution=2f/s.
The real-time image were evaluated objectively and subjectively. For objective scoring, the image signal-to-noise ratio (SNR), contrast noise ratio (CNR), geometric distortion and image uniformity obtained by the two sequences were measured. The signal intensity and noise at different positions of the image were measured and their average value was taken to calculate the SNR. The SNR is calculated by:
SNR=Signalnormal saline/SDnoise. The CNR between gadolinium-filled balloon and normal saline in the phantom was measured. The CNR is calculated by: CNR=|Signalballoon-Signalnormal saline|/SDnoise. Regarding image uniformity, most areas of multiple images were measured, and the average value of their uniformity was calculated. The image uniformity is calculated by: U={1-(Signalmax-Signalmin/Signalmax+Signalmin)}*100%. In terms of geometric distortion, measure the actual length of the gadolinium balloon and its length in the image, and then calculate the geometric distortion. The geometric distortion is calculated by: GD=|Lengthimage-Lengthactual|/Lengthimage*100%.
Subjective scoring of two sequences, Likert scoring method was applied to assess the image sharpness, image distortion and artifacts of all sequences. The images were scored by two experienced radiologists with more than six-year practice. The evaluation criteria were as follows: 1 points = poor image sharpness with serious distortion or artifacts, 2 points = medium image sharpness with medium distortion or artifact, 3 points = good image sharpness with slight distortion or artifacts, 4 points = excellent image sharpness with no distortion or artifacts. Independent sample T-test was used to analyze the scores of subjective evaluation.
Results: Both sequences temporal resolution was 2 frames/s and spatial resolution was 1.1×1.1×10mm. For objective assessment, the two sequences (FLASH vs True FISP) did show significant difference in SNR (102±16 vs 618±137, p<0.05) and CNR (73.5±18 vs 162.2±46,p<0.05). Image uniformity (80%±6% vs 74%±4%, p=0.133) and geometric distortion (2%±1%, 2%±1%) did not show significant difference. Subjective scoring showed that two radiologists reached agreement on the score after discussion, the subjective scores of the two groups of images did show significant difference, and the FLASH score is slightly higher than the True FISP score (FALSH=3.7±0.5, True FISP=3.1±0.9, P=0.03).
Conclusions: Both sequences have sufficient signal-to-noise ratio, contrast to noise ratio, image uniformity and the degree of geometric distortion is also within the acceptable range. The FLASH sequence has sufficient signal-to-noise ratio, and has sufficient guiding ability in the actual application process, the MR-compatible guide wire has moderate size of the marker artifact, and the balloon imaging effect is excellent. The True FISP sequence has higher signal-to-noise ratio and contrast-to-noise ratio, but the markers of the MR-compatible guide wire are marked with excessive artifacts, which affects the visualization of balloon and the vessel wall. The result of subjective evaluation shows that the FLASH sequence has a higher score than the True FISP sequence. Finally, the study shows that FLASH sequence has better guiding ability and effect compared with True FISP.
Fig.1
a-c: image of FLASH, a: guide wire, b: guide wire + balloon with Gd, c: balloon with Gd.
d-f: image of True FISP, d: guide wire, e: guide wire + balloon with Gd, f: balloon with Gd.
Fig.2
A: aorta phantom, B: balloon, C: MR compatible guide wire.
关键字
Interventional MRI,real-time imaging sequences,3D printed,image quality
报告人

发表评论